Commentary
Recently, Dr. Olaf Blanke, a Scandinavian neurologist, elicited an Out-Of-Body
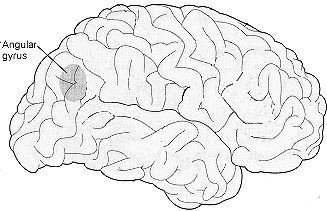
experience (OBE) for an epileptic woman when he stimulated the surface of her brain, in an area called the angular
gyrus.
One explanation for OBEs includes the idea that they
represent a very unusual activation of our spatial perception. In this explanation, a person who's having an OBE
perceives themselves as having a different location in space than their body. If this model is valid, then a disturbance
in any one of the brain areas responsible for spatial perception may also be implicated in out of body experiences.
The angular gyrus is small area in the temporal-parietal-occipital region of brain's surface. One possibility is
that the epileptic who was having an out of body experience in this study was one whose seizural activity included
the angular gyrus. That particular area of their brain may have been more sensitive than other areas ( that might
also contribute to the experience).
There are other areas that contribute to OBEs.
One of them is the hippocampus, and the other is an area of the brain's cortex which is directly connected to the
hippocampus called the parahippocampal region.
|
|
Blanke's observation points to only one area on the surface of the brain
- the angular gyrus. The angular gyrus is thought to participate in the brain's analysis of sensory information
that allows us to perceive our own bodies. When it misfires, Blanke suggested, the effects can include a sense
of floating, and/or seeing the world from a perspective outside of the body. While the angular gyrus is involved in our perception of our own bodies, its function in this
regard does not exclude other brain structures from also being involved.
|
Although the mechanisms behind body experiences are
not fully understood, Blanke's seems to imply that there is less known than is the case. Some participants in the
Shakti project, as well as many research subjects at Laurentian University's Behavioral Neurosciences program have
had out of body experiences following low intensity magnetic brain stimulation. While the evidence does not yet
allow a complete picture of the mechanisms of the out of body experience to be formulated, it does remove it from
the realm of total mystery.
One psychologist with the Skeptic Society, Dr. Michael Sherner, commented:
"Since all of our brains are wired in a similar manner, there is no reason to think that stimulation of this
brain region in other patients will not corroborate the finding."
This suggests that stimulating this brain region
of in other people may not reproduce Blanke's results. If stimulation of the angular gyrus did not produce out
of body experiences, there would still be other areas of the brain that might. If and when Blanke's results experiment
are replicated, the final result may be that there are several areas of the brain which can produce out of body
experiences on stimulation. A negative result from the Angular Gyrus would not be conclusive.
In the 1950's, the Canadian neurosurgeon Wilder Penfield
also succeeded in eliciting an out of body experience using electrical stimulation, but he was stimulating a very
different area of the brain, the sylvian fissure. The sylvian fissure divides the temporal lobes from the rest
of the brain along its length.. Dr. Michael Persinger has elicited out of body experiences through stimulation
of the temporal lobes using magnetic signals derived from the EEG signature of one of the structures deep in the
temporal lobes. Clearly, there is not a single "brain center" that supports out of body experiences but
rather a widely-distributed set of pathways. An individual's unique neural history leave any one of these most
likely to produce the experience for that individual.
|

|
A person, stimulating their Angular Gyrus without
effect may find that another area can facilitate out-of-body experiences for them because it will fire more easily.
If there are several areas that contribute to OBEs, then the one with the lowest thresholds will be the one most
likely to trigger one when that area is stimulated.
Blanke also reported that during the same session, the patient screamed, because she "saw" her legs shortening,
and "saw" her knees about to hit her face.
|
|
|
This experience is very similar to an experience called "micropsia",
in which a person may experience things as being closer than they really are. The opposite experience, called 'macropsia'
is the name for the perception that things are larger and farther away than they actually are. The same areas of
the brain we are discussing here are also involved in this experience. This writer has personally experienced macropsia
as preceding OBEs.
|
|
These pictures show where to put the coils to recruit
all the areas implicated in OBEs by the work of several researchers.
|
Magnetic Brain Stimulation, directed towards the
angular gyrus, the temporal lobes, the hippocampus, or the parahippocampal regions of the brain may have a chance
of making this experience available to all. Not all people would be equally prone to the experience, even with
correctly targeted stimulation.
|
|

|
These illustrations show the arrangement
of the coils for learning to have OBEs (much more likely after a session, while in twilight sleep) using four coils
only from the 8-Coil Shakti.
|
Even though we are interpreting Dr. Blanke's work on OBEs differently here, it nevertheless constitutes a substantial
step forward in our ability to understand out-of- body experiences and to induce them.
And now to the heart of the matter. How to use Shakti to increase your chances for having an OBE. NEXT
USING Shakti For Windows TO INCREASE YOUR CHANCES FOR HAVING AN OBE
SESSION DESIGNS
There are several areas of the brain (and several signals) that may increase your chances for having an OBE. One
of them is the Angular
Gyrus on the right side, another is
the temporal lobes on the right side, and another is the area where the occipital lobe, temporal lobe and parietal
lobe meet on the right side. In spite of the attention given to the angular gyrus on the right side following Dr.
Olaf Blanke's accidental elicitation of an OBE,
The most likely signal is the modulated 40hz signal. The second most likely is the Event-related potential signal,
especially over the angular gyrus, and the third most likely is the hippocampal signal.
|
Modulated 40hz signal
|
|
Tested by one experienced out-of-body practitioner who reported that
it elicited one of the sensations that precede OBEs during a short preliminary session.
|
|
|
|
|
|
Event-Related Potential Signal
|
|
Although it has NOT been tested yet, in principle the Event-Related Potential
signal may be able to initiate an event at the cortex (brain's surface). If this signal is applied over the angular
gyrus, that event could be an OBE, or another experience that may increase your chances for an OBE. They often
begin with a 'floating' sensation, or even a visual phenomena (macropsia) in which things seem farther away, or
(micropsia) closer than they actually are.
|
|
|
|
|
|
Hippocampal signal
|
|
The right hippocampus, with it's contributions to spatial perception
may contribute to OBEs, which involve a change in one's perceptions of one's location in space. The Hippocampal
signal is implicated in a small number of OBEs reported by participants in the Shakti Project, where only it and
the amygdaloid signal were used.
|
Cautions
This approach to having OBEs will involve stimulating only the right side of the
brain, and stimulating the temporal lobes more then the frontal lobes.
A good balance between the frontal lobes and the temporal lobes is important in
maintaining a healthy inner state. Do not do more than two series of sessions over the sides of your head in a
row. Alternate with series of sessions over the front of your head.
The first signs that you have stimulated your right hemisphere too much are feeling
low energy, sadness without cause, and/or periods of anxiety. Another sign that may occur is finding yourself having
trouble recalling words - the "word on the tip of your tongue that you just can't get out"
If you experience these things, you can apply the same signal to the same place
on the opposite side of your head. If these follow sessions with the hippocampal signal on the right side, you
may also correct them with the amygdaloid signal over the left side.